
Posters withdrawn: #2, #4, #10, #13,
#15
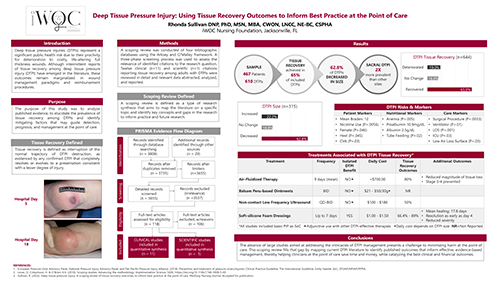
Deep Tissue Pressure Injury: Using Tissue Recovery Outcomes to Inform Best Practice at the Point of Care
Category: Research
Affiliation: iWOC Nursing Foundation, Jacksonville, FL
Abstract: Background: Deep tissue pressure injuries (DTPIs) represent a significant public health risk due to their propensity for deterioration to costly, life-altering full thickness wounds. Although intermittent reports of deep tissue pressure injury (DTPI) tissue recovery have emerged, these remain marginalized in wound management paradigms and reimbursement procedures. Purpose: The purpose of this study was to analyze published evidence, to elucidate the prevalence of DTPI tissue recovery and identify effective interventions to guide detection, prognosis, and management at the point of care. Methods: A three-phase scoping review was conducted using the Arksey and O’Malley framework. Twelve clinical (n=11) and scientific (n=1) citations reporting DTPI tissue recovery among adults were reviewed in detail and relevant data abstracted, analyzed, and reported. Results: The data was analyzed across a total sample of 467 adult patients with 610 DTPIs. Statistically significant risk factors and nutritional markers were identified. Primary DTPI locations were the sacrum (48.7%) and heel (23.8%). Tissue recovery was reported for 65% of the DTPIs with complete resolution occurring between 4 and 16 days. DTPIs decreased in size 62.8% of the time. Treatments associated with DTPI recovery included balsam Peru-based ointments, air-fluidized support surfaces, soft-silicone multi-layer border foam dressings, and non-contact low frequency ultrasound. Conclusion: This review of DTPI tissue recovery and DTPI-effective therapies, over a large and diverse sample, provides valuable insights into strategies that healthcare professionals can employ at the point-of-care, to achieve optimal clinical outcomes. Although much remains unknown and what is known suggests that DTPI evolution includes a trajectory towards full thickness tissue loss; this study demonstrates that tissue recovery is not only achievable, but common. Key contributors to successful outcomes were early identification and evidence-based interventions.
![]()
#18
Giant Omphalocele and the Challenges of Healing and Containment: A Case Study
Category: Case Study
Affiliation: UNC Health, Chapel Hill, NC
Abstract: Problem Statement:: Giant omphalocele (GO) is a rare (incidence of about 1/6000 live births) midline ventral wall defect with herniation of viscera into a sac and is associated with high rates of mortality and morbidity. We present a former 35-week gestation, 2650 gram/5.8-pound birthweight 8-week-old female with GO complicated by infection, pressure injuries, cellulitis of stalk (base of GO), pain, and pulmonary hypoplasia. Stabilization was difficult, size (20x43cm) and skin fragility of the GO were intimidating. She was referred to the care of the WOC team. Significance to Practice/Past Management: There is no accepted standard for the care of a GO or its ‘skin’. Past treatments involved escharotic agents such as silver sulfadiazine, silver nitrate, and povidone-iodine which we did not employ due to pain, risk of silver toxicity, and potential thyroid dysfunction in this compromised infant. Compression was not an option due to the 19cm stalk. Solution/Clinical Treatment Approach: A multidisciplinary plan of care was tailored to meet the dynamic needs of the infant as well as simplicity for staff. We utilized an array of advanced wound products beginning with a silicone non-adherent contact layer to a highly absorbent non-bordered silicone foam to finally a Pva-Gentian Violet-Methyl Blue foam. The GO was contained with a patient specific garment sewn out of a soft tissue support bandage, supported by a foam stabilizer and fluidized positioner. Outcomes/Conclusion: The WOC team performed twice a week dressing changes and collaborated with the OT team during the entire admission. This lessened the need for pain medication, decreased episodes of bradycardia/desaturation, and reduced staffing needs for caring for the patient from 4 to 1. The outer layer of the GO ‘skin’ healed in 4 months. This improved the stability of the GO during transfers, enabled ‘tummy time’ for overall developmental skills acquisition, and the GO progressed to a manageable discharge status. There are alternatives to escharotic agents with effective outcomes. The authors concluded that a soft tissue support bandage is an effective containment device for GO babies that are not surgical candidates.
![]()

#6:
A New Bordered Foam Dressing Technology Improves Wound Outcomes and Satisfaction While Reducing Dressing Utilization in Acute Care
Category: Practice Innovation
Affiliation: Cookeville Regional Medical Center, Cookeville, TN
Abstract: Objective: Empirically, we observed peri-wound maceration, epidermal stripping, and poor adhesion with the bordered foam dressing on formulary. We converted our entire bordered foam dressing formulary to a newly redesigned dressing with enhanced absorption and greater flex with movement. The new design enabled us to change the policy for routine dressing changes from every 3 days to every 7 days. Method: We compared similar periods pre and post implementation of the new dressing to determine the impact of efficiency of the new dressing design on the number of dressing changes per patient, clinical outcomes, and patient/staff satisfaction. Results: 5 patients with 10 wounds had length of stay during which WOC nurse assessed the wound more than once which enabled evaluation of dressing performance and wound volume reduction. 7 of the 10 wounds achieved 57.8% reduction in wound volume (average 67% progression wound healing). Wound nurse and staff evaluations indicated that new dressing absorbed better, adhered without medical adhesive-related skin damage and improved patient comfort. Dressing utilization per patient for the quarter following full implementation of the new formulary was reduced in comparison to the utilization with prior formulary. Extending the dressing wear time required re-educating staff with focus on undisturbed wound healing. Processes utilized to support the change in practice included extensive education: on-line and at bedside. A multi-disciplinary skin champion team was formed to augment education and best practice. EMR prompts were updated to facilitate the selection of clinical basis for dressing change outside of the protocol. Conclusion: Converting our wound care formulary to single, more efficient, flexible bordered foam dressing improved patient healing outcomes, patient, staff and WOC satisfaction and reduced the number of dressings utilized per patient.
![]()

#01:
Use of Polyurethane Foam Containing Methylene Blue, Gentian Violet, and Silver in the Treatment of Chronic Wounds
Category: Case Study
Affiliation: Florida International University, Miami, FL
Abstract: Background: Chronic wounds occur when disrupted repair processes occur in one or more stages of wound healing. Current estimates indicate that as many as 8.2 million Americans have a chronic wound. Management of chronic wounds has an average annual cost of $96.8 billion. Purpose: This case series provides an overview of five patients with unique chronic wounds in various stages of healing that were treated with a polyurethane foam dressing containing methylene blue, gentian violet, and silver. This dressing can be utilized throughout the healing process. Our clinical case series reveals the versatility of this approach to chronic wound care. Methodology: The methodology for this project involved a case series design including five patients who presented with unique wounds for 12 to 16 weeks before being referred for advanced wound care services. Prior to advanced wound care referral, four cases were treated by primary care providers. One patient was referred as a result of post-surgical wound complications. Results: The case series includes a review of the healing trajectories of all five patients to wound closure between 4- and 8-weeks post-referral. Conclusions: Silver wound dressings generally have broad antimicrobial effectiveness. The addition of methylene blue and gentian violet appears to broaden antimicrobial coverage. Furthermore, foam dressings are able to manage moderate-to-highly exudative wounds. Results from this case series demonstrate the utility of the chosen intervention and suggest that polyurethane foam dressing containing methylene blue, gentian violet, and silver may be a viable intervention for first-line treatment for a broad range of chronic wounds.
![]()

#3:
Evaluation of Wound Bed Preparation with Monofilament Pad
Category: Case Study
Affiliation: Wellstar Spalding Regional Hospital, Griffin, GA
Abstract: Clinical Problem: Bedside debridement challenges include scope of practice, cost, and provider time. Discomfort from infection and anticoagulation therapy are often barriers to providers lacking scope or access for sharp debridement. Sharp debridement is not always the best option for wound bed preparation. Past Management: Conservative sharp debridement is the standard method for removal of slough and loose debris but is not always available due to scope of practice. Modalities like ultrasonic debridement require equipment and supplies that are not always readily accessible. Effective topical therapies will take longer than methods that immediately remove debris. Current Clinical Approach: A disposable debriding pad or lolly consisting of monofilament polyester fibres was used for wound bed preparation when slough and /or scaling was present. The device was used to debride the necrotic tissue or scales for 30 seconds to 2 minutes, dependent upon patient tolerance. Patient Outcomes: Patients #1-4 were treated with device for 2 minutes; patients #5 and #6 for 30 seconds x 2 due to tenderness in wound bed. Patient #1, #2 and #3, neuropathic feet: wound beds visibly cleaner, #2 loosened tissue for sharps debridement; # 3 scaling markedly improved and wound bed well defined; Pt #4 100% dense adherent slough showed visible disruption in wound bed, 15% clean after treatment; Pt #5 scaling resolved and wound bed beefier and hydrated; Pt #6 wound bed 50% slough removed allowing some sharp debridement to be completed. Conclusions: Skin scaling: removed atraumatically and comfortably. Debridement: When discomfort was present it was well tolerated with a short rest period; appears to break up the density of the tissue surface for penetration of topicals; some slough loosened up well enough to sharp debride; well tolerated in neuropathic patients. Bleeding: None associated with use. As no sharp debridement is utilized, the monofilament is a safe, inexpensive, and effective debridement option for multiple care settings.
![]()

#5: (Non judged - Board Member)
Using Convexity in the Management of Complex Clinical Challenges
Category: Practice Innovation
Affiliation: Moffitt Cancer Center, Tampa, FL
Abstract: The use of convexity in challenging clinical situations requires versatility to improve patient outcomes. Utilizing convex rings proved to be beneficial in managing multiple complex cases. WOC nurses selected durable and flexible convex rings designed to prevent leakage and heal the altered skin of patients with a neck fistula, retracted urostomy and a leaking gastrostomy tube. Positive results were measured with skin protection, patient comfort, accurate measurement of drainage output; ease of use by clinician, and optimization of nursing time. Being creative with products and techniques helped WOC nurses trouble-shoot and succeed to meet oncology patients' care needs.

#7:
Implementing a Protocol to Prevent Skin Breakdown with Prolonged Use of N95 Masks and other Surgical Masks
Category: Practice Innovation
Affiliation: Grady Memorial Hospital, Atlanta, GA
Abstract: Introduction: The skin is the first line of defense and serves in different functions. The skin acts as barrier protecting the body against harmful external forces. Pressure injures (PI) develop from constant pressure, shear/friction, and moisture. Despite the protection these devices provide, constant use of personal protective equipment (PPE) for long period of time 8 to 12 hours may cause pressure to different areas the face such as nose bridge and checks, which can lead to partial-thickness skin damage, bruising and dermatitis. They can also cause discomfort and additional stress to healthcare employees. However, PPE equipment is necessary to protect healthcare workers from the COVID-19 virus. Purpose: To decrease skin breakdown due to prolonged wear of N95 masks and other surgical masks in healthcare workers. Methods: Distribution and education on proper use prior to application of the N95 masks and other surgical masks and how to care for the skin post mask removal. Results: There were decreased facial skin breakdown, bruising and dermatitis on healthcare workers’ faces. Conclusion: Developing and implementation of protocols can effectively decrease and prevent skin breakdown, pain, and discomfort from prolonged use of N95 masks and other surgical face masks in healthcare workers.
![]()

#8:
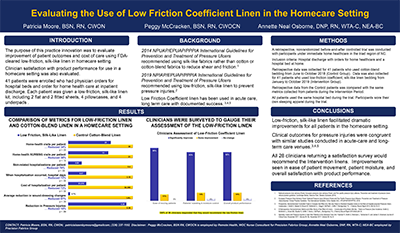
Evaluating the Use of Low Friction Coefficient Linen in the Homecare Setting
Category: Research
Affiliation: Advanced Home Health, High Point, NC; Adoration Home Health, Wise, VA; Precision Fabrics Group, Greensboro, NC
Abstract: Introduction: EPUAP/NPIAP/PPPIA International Guideline for the Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline-2019, Preventive Skin Care section recommends to “consider using textiles with low friction coefficients for individuals with or at risk of pressure injuries. (Strength of Evidence = B1)” Purpose: The purpose of this practice innovation was to evaluate improvement of patient outcomes and the cost of care using FDA cleared low friction coefficient linen in the homecare setting. Method: Fifty patients were enrolled who had a physician order for Skilled Home Health and a hospital bed at inpatient discharge. Each patient was given a silk-like, low friction coefficient linen kit that included 2 flat sheets, 2 fitted sheets, 4 pillowcases and 4 medium underpads. The clinical data collection period was from January 2019 to October 2019. Review of the patients EMRs yielded data pertaining to pressure injury stages and measurements, rehospitalizations, home visits by clinical staff and supply costs. This data was compared to a similar patient population who met the inclusion criteria from the previous 6 months. This data was analyzed using a Paired Sample T-test. Results: Nursing visits were reduced by 42% with a P- value of 0.12. Total visits including all disciplines were reduced by 34% with a P- value of 0.03. Rehospitalizations for skin related causes were reduced by 81%. Furthermore, these results reduced the total cost of care. Conclusion: Patented and FDA cleared silk-like, low friction coefficient linen facilitated dramatic improvement in patient outcomes in all patients using low friction coefficient linen at home. Clinical outcomes for Pressure Injuries are congruent with similar studies conducted in acute care and long-term care venues.
![]()
#9:
Effects of a Spinal Stabilization Table (SST) on Pressure Injury Development in the Acute Adult Spinal Cord Injury Patient
Category: Research
Affiliation: University of Florida Health Jacksonville, Jacksonville, FL
Abstract: Background: According to the AHQR (Agency for Healthcare Quality and Research) “Pressure ulcers (now known as pressure injuries) cost $9.1-$11.6 billion per year in the U.S., Cost of individual patient care ranges from $20,900- $151,700 per pressure ulcer.” Medicare estimated in 2007 that each pressure ulcer added $43,180 in costs to hospital stays. Spinal cord injury (SCI) patients have a 6-46% increase in incidence of developing pressure injuries due to changes in micro-circulation and decreased blood flow to the tissues. According to Courtney Lyder, pressure injuries can develop in as little as two hours of admission to the hospital in the high-risk acute SCI patient population. Upon the request of a Trauma Resident some twenty-nine years ago, I modified the seat hatch section of a Spinal stabilization table (SST) in a trial to reduce skin breakdown over the sacral/coccyx areas of this high-risk population. Methods: A retrospective study was completed that included a total of 48 patients. Two separate Surgical Intensive Care Units (SICUs) were studied. Thirty-nine patients in the control group who utilized the standardized manufacturer’s seat hatch cushion (control group) nine patients in the adjacent SICU comprised the experimental group. The experimental group utilized the replacement modified four-inch-high density foam cushion (FIHDFC). Data was collected for 59 months (February 2012-January 2017). Results: Of the total forty-eight patient population, fourteen of thirty-nine patients in the control group developed at least one pressure injury. Three patients in this group developed a pressure injury within the first two days of placement on the SST. The total time of placement on the SST for the control group ranged from one to thirty-three days. The percentage of breakdown was 28% in the control group. The experimental group remained on the SST from one to twenty-seven days prior to spinal stabilization surgery. Unfortunately, one patient in the control group who was in his sixties developed a Stage 4 on day fourteen on the SST. This pressure injury was subsequently debrided to bone requiring placement of a wound vac prior to his spinal fusion surgery. Another patient in his sixties (experimental group) was on the SST with the replacement FIHDFC for twenty-seven days. He was able to go to surgery with no pressure injury in his sacral/coccyx region. Conclusion: Utilization of a replacement FIHDFC in the seat hatch of the SST greatly reduces the incidence of pressure injury development in the acute adult SCI population.
![]()

#11:
Empowering Patient Care Technicians to Support a Healthcare System's Interprofessional Wound Care Protocol
Category: Practice Innovation
Affiliation: Baptist Health, Montgomery, AL
Abstract: Background: Wound, skin, and tissue health accountability falls on all healthcare team members; physicians, nurses, physical therapists, dieticians, and respiratory therapists. The primary nurse is often focused on the admission diagnoses not necessarily related to skin and wound issues. However, the Patient Care Technician (PCT) is often the initial caregiver in this medical setting to provide personal care for the patient. Setting: 650 bed acute care health system consisting of three hospitals. Purpose: Recognizing the PCT’s vital role as a “front line” provider, this health system decided to be inclusive of all who come in contact with our patients and provide in-depth education to empower PCTs with the tools to partner in skin care. Method: A systematic approach to educate PCTs to identify and manage high risk patients, within their scope of practice, and how to communicate their findings was developed in an effort to promote early detection and prevention of pressure injuries and skin damage related to other etiologies. WOC nurses present a ninety-minute introduction to skin damage identification and treatment options during PCT orientation. After six months of employment, PCTs are eligible for an increase to their hourly pay rate through participation in a clinical ladder program designed to increase their knowledge and skills for effective patient care related to skin health. Results: Within the last five years, more than 400 PCTs have participated in education classes. Topics include offerings in skin damage identification, pressure injury prevention, and appropriate product use. Conclusions: This collaboration has fostered teamwork and mutual respect amongst caregivers to ensure effective and timely patient care. In the future, we aspire to link objective patient outcome data to our initiative and demonstrate that interprofessional skin and wound care programs which also include PCTs have a positive impact on patient outcomes related to skin health.
![]()

#12:
The Ostomy Lift: An Innovative Technique to Decrease Peristomal Skin Creases and Increase Wear Time of the Pouching System or Ostomy Barrier
Category: Practice Innovation
Affiliation: Self, Boynton Beach, FL
Abstract: Leakage from an ostomy effects up to 87% of ostomates and is associated in patients with an elevated Body Mass Index (BMI). Ostomy leakage causes great distress and contributes to a poor quality of life. Peristomal skin creases are common in obese individuals and contributes to pouch leakage. Ostomy lift is an innovative technique using kinesiology tape to minimize peristomal creases and subsequently reduce leaks by reshaping and remolding skin folds. This poster presents a case study of an innovative technique, of how kinesiology tape can be used to reduce creases and decrease ostomy leaks. A 37-year-old obese male (BMI 33%) presents with a transverse colostomy located in the left upper quadrant. The stoma protrudes slightly, and the lumen touches the skin at 6 o’clock. Deep creases were seen at 10 and 3 o’clock when seated, and the stoma retracted. Barriers were leaking daily causing peristomal skin damage, anxiety, and depression. The certified WOC nurse made several home visits to troubleshoot and change the leaking ostomy appliance. Various appliances, belts and caulks were trialed without success and great frustration. After exhausting all conventional tactics, kinesiology tape was placed on the skin above the stoma to lift the belly flesh thereby flattening the deep creases. The ostomy lift technique was successful in reducing the creases and obtaining a seal. The patient states the kinesiology tape feels comfortable and the ostomy appliance feels supported. Leaks are now uncommon and wear time is 3-5 days. While this is one unique case, it is an exciting innovation that may be helpful for those ostomates who suffer from chronic leaks due to deep peristomal creases.
![]()

#14: (Non judged - Board member)
14. Improving the Accuracy of Pressure Injury Reporting
Category: Practice Innovation
Affiliation: Medical University of South Carolina, Charleston, SC
Abstract: At an 825-bed academic medical center in the Southeast, hospital-acquired pressure injury (HAPI) rates are on the rise. Research has found that the former method of reporting at this institution (through an electronic health record report) was inaccurate, causing missed pressure injury prevention (PIP) opportunities. Namely, the wound care nurse team was not aware of some pressure injuries. Through improved reporting, the goal is to reduce patient harm and reduce healthcare costs. These aims come from early intervention and improved bedside coaching on high HAPI units. The Pressure Injury Preventionist, a certified wound care nurse dedicated to pressure injury prevention and reducing HAPI rates, has been key in reshaping and reforming our former model of reporting pressure injuries through process improvement. Our new model utilizes the following multi-pronged approach: 1) certified wound care nurses monitor and record all pressure injuries, 2) when a HAPI is identified and documented, a huddle with bedside care team members occurs in real-time to coach and correct any outstanding prevention elements and missed opportunities on the unit, 3) this is followed by an Apparent Cause Analysis (ACA) with bedside care team members and nursing leadership to identify strengths, gaps, and opportunities. Recently, these ACAs have led to a trial of a different brand of heel suspension boots for patients identified at-risk or identified with a PI. There is also an increase in buy-in from nursing leadership thanks to this streamlined, multi-pronged approach to pressure injury reporting. Research is on-going as to whether HAPI rates will decrease.
![]()

#16
Prophylactic Dressings: Are They Barriers to Assessment?
Category: Practice Innovation
Affiliation: Wellstar Spalding Regional Hospital, Griffin, GA
Abstract: Introduction: Worldwide no known standards exist for prophylactic dressings, despite their international widespread and growing use. Performance standards based on bioengineering laboratory testing generate critical information which is needed to guide effective medical product selection and practice. In March 2021 the National Pressure Injury Advisory Panel started the Prophylactic Dressing Standards Initiative (PDSI) with establishment of a dedicated international Task force to evaluate standards for use. From January 1 to February 18, 2020, there were six identified hospital-acquired sacral pressure injuries (PIs) in the ICU. Two of these appeared to be the shape of the prophylactic dressing. Per the ICU’s PI prevention protocol prophylactic sacral foam dressings were initially implemented due to suboptimal support bed surfaces; despite ICU support surface replacement in 2018, prophylactic sacral foam dressings were still utilized. Analysis raised the question of whether prophylactic dressings were hindering the skin assessment process as frontline nurses acknowledged not lifting the prophylactic dressings for skin assessments as they were taught per the PIP protocols. Objectives: To evaluate if removing visual barriers, i.e., prophylactic dressings could impact the hospital-acquired sacral PI rates in ICU. Methodology: Sacral foam prophylactic dressings and adult diapers were identified as skin assessment barriers and were removed from ICU on February 19, 2020. The data collection was slated for 45 days but was cut short at 41 days due to COVID-19 impacting external factors, predominantly staffing. No additional staff education was provided other than the rationale for removing the sacral foam prophylactic dressings and adult diapers. Results: There were six identified hospital-acquired sacral PIs documented in the first 49 days of patient care compared to one in the subsequent 41-day period. Conclusion: The preliminary data indicates there is an opportunity to evaluate the need for placing a sacral prophylactic dressing on every at-risk patient when appropriate support surfaces are in place. Ideally, the data timeframe would have been longer to determine if there was a sustainable impact on lowering hospital-acquired PI incidence rates thereby supporting this evaluation’s objective, whether the removal of visual barriers aids in sacral PI reduction. Additionally, delivering alternative methods of PIP education should be explored. Potential topics could be how to complete a thorough skin assessment on patients utilizing a sacral prophylactic dressing.
![]()

#17
Hypochlorous Acid Wraps as a Precursor to Compression Therapy with Venous Stasis Ulcers
Category: Case Study
Affiliation: UNC Rex Healthcare, Raleigh, NC
Abstract: Background: Healing venous stasis ulcers can be a painful and time-consuming process. Compression is the gold standard of healing venous stasis ulcers, but many patients cannot tolerate any level of compression due to pain. Decreasing pain enough to begin healing wounds is an important and often difficult first step to achieve, making it so the patient may then tolerate compression therapy. Wet-to-moist therapy using hypochlorous acid wraps (HAW) has shown potential as a first step in healing venous stasis ulcers without initial use of compression. Healing venous stasis ulcers can be a painful and time-consuming process. Compression is the gold standard of healing venous stasis ulcers, but many patients cannot tolerate any level of compression due to pain. Decreasing pain enough to begin healing wounds is an important and often difficult first step to achieve, making it so the patient may then tolerate compression therapy. Wet-to-moist therapy using hypochlorous acid wraps (HAW) has shown potential as a first step in healing venous stasis ulcers without initial use of compression. Methods: A case study of three inpatients has shown that using HAW can be an effective way to begin the healing process for venous stasis ulcers. The method used for application consists of a) saturating gauze wrap with moistened hypochlorous acid, b) wrapping the moistened gauze around the affected lower extremity, c) applying ABD pads over moistened gauze, d) wrapping with dry gauze to keep dressing in place, and e) securing with perforated tape (not placing tape on skin) to hold dressing in place. This dressing is then changed every 12 hours, reflecting the half-life of hypochlorous acid. Results: In this three-patient case study, the venous stasis ulcers showed a decrease in size, decrease dead tissue on the wound beds, and a decrease in pain. Conclusion: With consistent twice daily dressing changes using HAW, venous stasis ulcers can heal more quickly and with less pain. This helps to promote patient comfort and compliance with subsequent compression therapy. A case study of three inpatients has shown that using HAW can be an effective way to begin the healing process for venous stasis ulcers. The method used for application consists of a) saturating gauze wrap with moistened hypochlorous acid, b) wrapping the moistened gauze around the affected lower extremity, c) applying ABD pads over moistened gauze, d) wrapping with dry gauze to keep dressing in place, and e) securing with perforated tape (not placing tape on skin) to hold dressing in place. This dressing is then changed every 12 hours, reflecting the half-life of hypochlorous acid. Results: In this three-patient case study, the venous stasis ulcers showed a decrease in size, decrease dead tissue on the wound beds, and a decrease in pain. Conclusion: With consistent twice daily dressing changes using HAW, venous stasis ulcers can heal more quickly and with less pain. This helps to promote patient comfort and compliance with subsequent compression therapy.
![]()

#19
Taking the Load Off in Home Health Care: The Provision of Therapeutic Support Surfaces
Category: Practice Innovation
Affiliation: Amedisys Home Health, Senoia, GA, Apison, TN, St. George, SC
Abstract: Pressure relief in home health patients often falls short of best practices despite years of published literature including the AHRQ regulations, NPIAP guidelines and WOCN Society guidelines. The authors objectives were to: (1) educate clinicians, (2) provide resources to streamline the delivery of the pressure relief support surfaces, and (3) develop a process to monitor skin integrity while utilizing pressure relief support surfaces. Our first step was to vet regional Durable Medical Equipment (DME) support surface providers to identify mutual goals. After multiple meetings with DME companies, an informal relationship was established with a regional DME who specializes in support surfaces only. The DME agreed to provide quality therapeutic equipment, productive communication with each home health care center and prompt delivery to the patients’ homes. With approval of our leadership, the program was launched. Concurrently, the WOCN Society Support Surface Algorithm was integrated into the OASIS documentation at corporate level. The Regional Wound Care Directors in the localities of the initiative along with the DME consultant partnered to educate the care center clinicians. An inservice was presented to each of the regional care centers on the WOCN Society Support Surface Algorithm, CMS regulations, company policy and the new streamlined process for acquiring the needed equipment. The DME consultant worked directly with the care center field staff, leadership, and the medical providers to ensure best practices were in place for the patients. The implementation of evidence-based practice for the utilization of support surfaces resulted in improved nursing knowledge, increased patient satisfaction and efficient product delivery to the patients’ homes. The outcome was an improvement in wound healing as evidenced by a decrease in the Wound Assessment Tool (WAT) Score and photographic documentation.
![]()

#20
Rectal Pouch: An External Option for Fecal Management During Prone Positioning Therapy
Category: Practice Innovation
Affiliation: University of Alabama at Birmingham Hospital, Birmingham, AL
Abstract: Background: In 2020, a Medical Intensive Care Unit at a large Southeast academic hospital was converted to a COVID-19 ICU. One of the treatments utilized for COVID-19 patients was prone positioning therapy. These prone patients were heavily sedated, sometimes paralyzed, to ensure ventilator compliance. Due to the deep level of sedation, prone patients became incontinent during therapy. Indwelling fecal containment systems, such as a bowel management system or a rectal tube, were used for these patients. The prone patients began having complications with the long-term use of these indwelling systems such as rectal and anal pressure injuries, some requiring gastroenterology interventions. Methods: For the patients with rectal or anal injuries, an external option was needed. The unit WOC nurse introduced the unit staff to a rectal pouch that could be applied externally around the anus. The pouches were used on prone patients who had acquired injuries internally or had low platelet counts. The unit WOC nurse also made an educational video for the staff nurses showing them how to properly apply a rectal pouch to a patient. Results: Prior to the implementation of the external rectal pouch, indwelling fecal containment systems were the only options available to the nursing staff. After the educational video on rectal pouch application, the nursing staff felt more confident on applying the pouches themselves. This led to the external rectal pouch becoming the first choice of fecal containment systems for prone patients, as opposed to the indwelling options. Conclusion: With the implementation of the external rectal pouch, the use of internal fecal containment systems decreased significantly as well as the number of device related pressure injuries.
![]()

#21
Usability Testing of the Patient Reported Outcomes-Informed Symptom Management System: a personalized mHealth Program
Category: Research
Affiliation: UNC School of Nursing, Chapel Hill, NC
Abstract: Background: Cancer patients and their caregivers often receive education about ostomy care during hospital stay for ostomy surgery. However, most patients struggle with ostomy care after being discharged home, causing complications and symptoms (e.g., dehydration and peristomal skin breakdown) that lead to readmission and emergency room use. These complications and symptoms are preventable with appropriate self-/family-management. This study aimed to test the usability of our newly developed Patient Reported Outcome-Informed Symptom Management System (PRISMS) an innovative web-based mHealth program that helps complications and symptoms self-management during transition from in-patient professional care to post-treatment self-care at home. Methods: The usability testing was comprised of two phases. In Phase I, two rounds of focus groups were conducted among healthcare providers. In Phase II, cancer patients with newly created ostomies and their caregivers were interviewed in a research lab; each participant performed three tasks on the PRISMS prototype: doing a Patient-Reported Outcomes (PRO) survey, exploring the dashboard, and watching a skills-training video. The SMI Eye Tracking Glasses were used to collect gaze data during the tasks. In addition, each participant completed the eHealth Literacy Scale survey and a qualitative interview. Results: Eight healthcare providers provided comments and feedback on the PRISMS contents and mode of delivery. Six patients and three caregivers participated in the Phase II usability testing. Five categories of feedback were identified from the analysis of the interviews: content, navigation, functionality, appearance, and intervention implementation related. Conclusion: Based on stakeholders’ feedback, we have comprehensively refined PRISMS and improved its functionality. Currently, we are conducting a pilot randomized clinical trial to test the feasibility of PRISMS in which a Wound and Ostomy Care nurse interventionist leverages the embedded PRO survey and smart devices data to monitor the postoperative complications and symptoms and provider support based on patients’ and their caregivers’ care needs.
![]()

#22
Does a Shorter Length of Use for a Fecal Containment Device Lower the Risk of Pressure Injuries?
Category: Research
Affiliation: University of Alabama at Birmingham Hospital, Birmingham, AL
Abstract: Background: The fecal containment device hospital policy for a Southeast academic hospital states: a fecal containment device, such as a bowel management system or rectal tube, can be used for 29 days. In the hospital medical intensive care unit, a correlation was observed between longer duration of use and the development of internal/external pressure injuries in the rectum and anus. The purpose of this study was to compare the device use to the development of internal or external pressure injuries. The time of use was decreased to 7 days for a bowel management system and 21 days for a rectal tube. Methods: The quasi-experimental study included MICU patients receiving prone positioning therapy and requiring a fecal management device. The decision of using a bowel management system versus a rectal tube was made based on consistency of fecal matter. For June 2020, 37 patients received prone positioning therapy and required a fecal containment device. Of the 37 patients, 25 required a bowel management system and 5 required a rectal tube. For the bowel management system, 16% (4 of 25 patients) developed an internal mucosal pressure injury. For the rectal tube, 20% (1 of 5 patients) developed an external pressure injury. Between July 13th and October 21st, 2020, 91 patients received prone positioning therapy. Results: Of the 91 MICU prone patients, 31 utilized a bowel management system and 46 utilized a rectal tube. For the bowel management system, 9.6% (3 of 31 patients) developed an external pressure injury and 0% developed an internal mucosal pressure injury. For the rectal tube, 2.17% (1 of 46 patients) developed an external pressure injury & 0% developed an internal mucosal pressure injury. Conclusions: With shorter lengths of use for fecal containment devices, there is a lower risk of developing an internal or external pressure injury on the rectum and anus.
![]()
