Poster #14
Optimizing Peri-Stomal Complications with New Technology
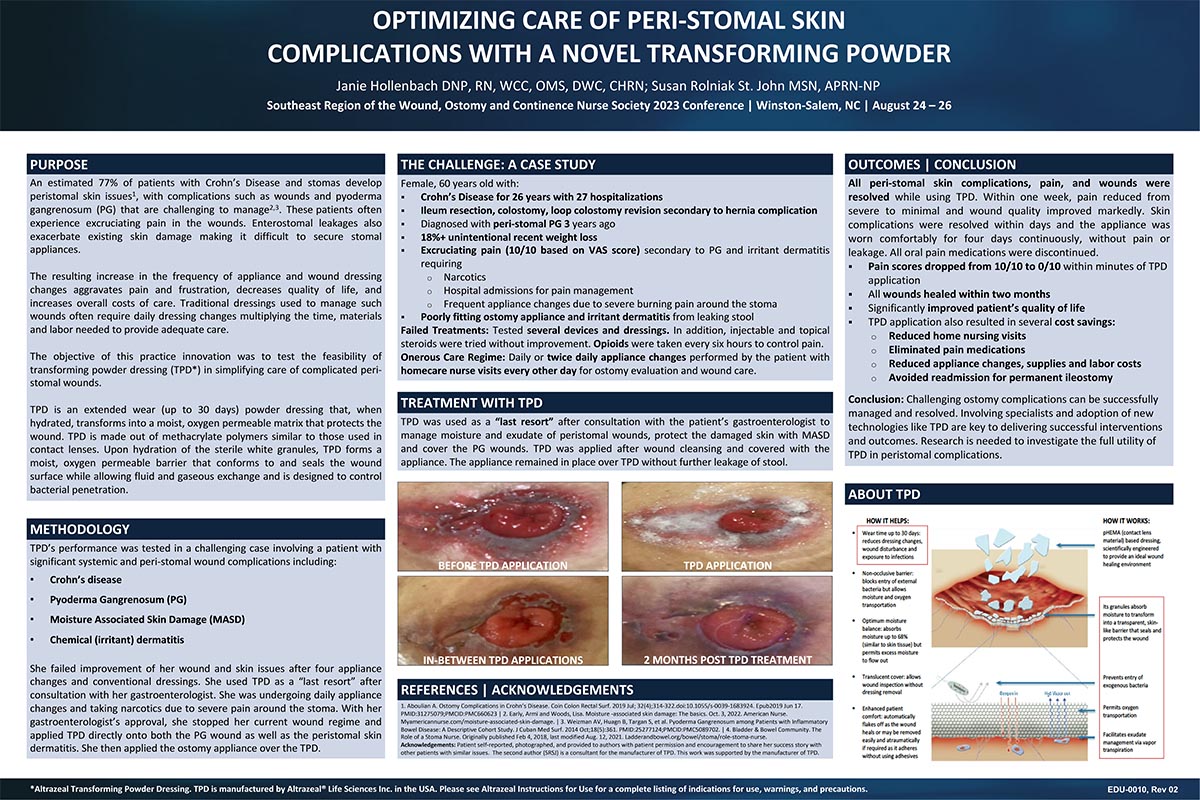
Abstract: Purpose: An estimated 77% of patients with Crohn’s Disease and stomas develop peristomal skin issues1, with complications such as wounds and pyoderma gangrenosum (PG) that are challenging to manage.2,3 Effluent leakage exacerbates existing skin damage making it difficult to secure stomal appliances. The objective of this practice innovation was to test the feasibility of transforming powder dressing (TPD) in simplifying care of complicated peri-stomal wounds. TPD is an extended wear (up to 30 days) powder dressing that, when hydrated, transforms into a moist, oxygen permeable matrix that protects the wound. TPD is made out of polymers similar to those used in contact lenses.
Methodology: 60 year-old female with Crohn’s Disease, colostomy s/p ileum resection, PG, moisture associated skin damage (MASD) who failed improvement after four appliance changes and conventional dressings/treatments used TPD as a “last resort” after consultation with her gastroenterologist. She was undergoing daily appliance changes and taking narcotics due to severe pain around the stoma. With her gastroenterologist's approval, she stopped her current wound regime and applied TPD directly onto both the PG wound as well as the peristomal skin dermatitis. She applied the ostomy appliance over the TPD.
Outcomes: All peri-stomal skin complications, pain and wounds were resolved within 2 months after TPD initiated. Skin complications (except for PG) were resolved within days and the appliance worked comfortably for 4 days continuously, without pain or leakage. Within 1 week, pain reduced from severe to minimal, and all oral pain medications were discontinued. For this patient, changing from conventional treatments to TPD resulted in 1) elimination of pain medications, 2) improved quality of life, 3) reduced home nursing visits, and 4) reduced appliance changes, supplies and labor costs. Involving specialists3 and adoption of new technologies like TPD are key to delivering successful outcomes.
![]()
Poster #15
Novel Treatment of an Enteroatmospheric Fistula with Transforming Powder Dressing (TPD)
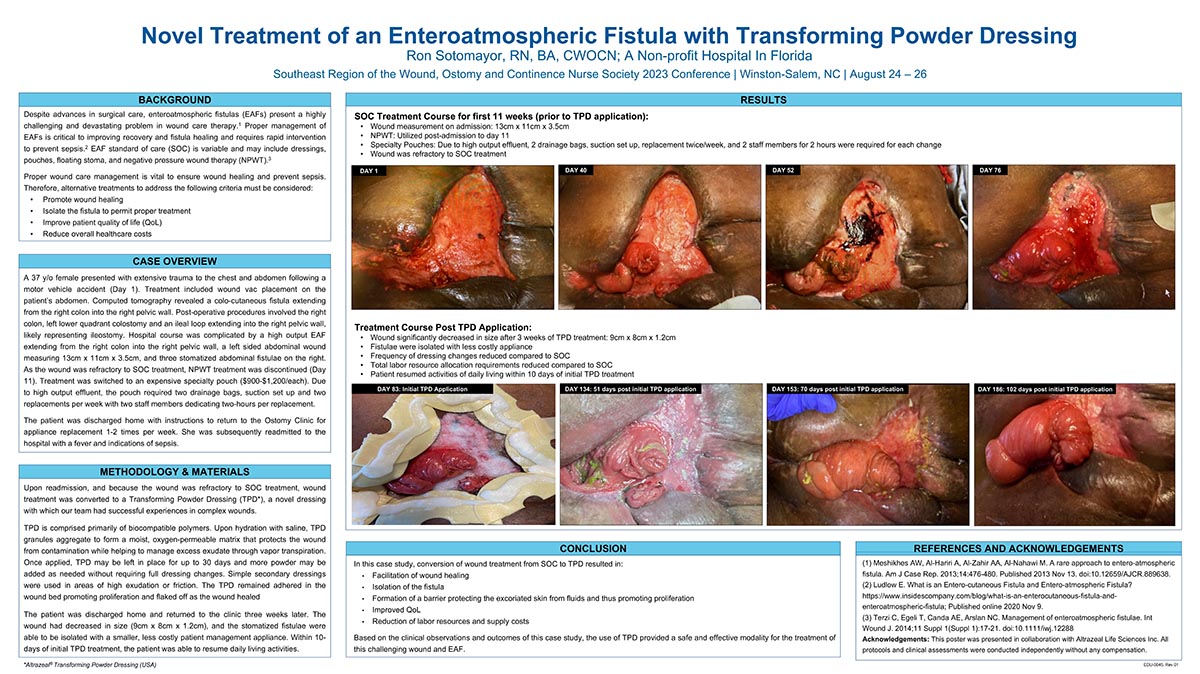
Abstract: Purpose: Despite advances in surgical care, enteroatmospheric fistulas (EAFs) present a highly challenging and devastating problem in wound care therapy.1 Proper management of EAFs is critical to improving recovery and fistula healing, and requires rapid intervention to prevent sepsis.2 EAF standard of care (SOC) is variable and may include dressings, pouches, floating stoma, and negative pressure wound therapy (NPWT).3 As proper wound care management is vital to ensure wound healing and prevent sepsis, consideration for alternative treatments which promote wound healing, isolate the fistula for proper treatment, improve quality of life (QoL), and reduce overall healthcare costs must be considered.
Methods: A 37-year-old female presented with extensive trauma to the chest and abdomen following a motor vehicle crash. Hospital course was complicated by a high output EAF extending from the right colon into the right pelvic wall, a left sided abdominal wound measuring 13cm x 11cm x 3.5cm, and three stomatized abdominal fistulae on the right.
In spite of the failures of current SOC used such as NPWT and specialty pouches, a transformative powder dressing (TPD) made of biocompatible polymers applied once a week which forms a layer of protective matrix proved to be an innovative advance in the epithelialization of the wound bed.
Results: The patient was discharged home and returned to the clinic three weeks later. The wound was observed to have decreased in size (9cm x 8cm x 1.2cm), and the stomatized fistulae were able to be isolated with a smaller, less costly patient management appliance. Within 10-days of initial TPD treatment, the patient was able to resume daily living activities.
Discussion: TPD is a novel dressing which our team has successfully used in complex wounds. Upon hydration, TPD aggregated on the wound and formed a moist, oxygen-permeable matrix that protected the wound from contamination and helped manage excess exudate. Secondary dressings were used in areas of high drainage.
Treatment with TPD resulted in the facilitation of wound healing, isolation of the fistula, improved QoL and a reduction in resource and supply costs. Based on the clinical observations and outcomes of this case study, use of TPD provided a safe and effective modality for the treatment of this challenging wound and EAF.
![]()
Poster #1
Use of a PVA Gelling Fiber to Heal Complex Wounds, Reduce Pain & Suffering, and Save Time: A Retrospective Review
Abstract: Background: Annually, wounds affect approximately 8.2 million people in the United States and cost the US $28.1 to $96.8 billion to treat. Much of this cost is unnecessary spending, related to delayed diagnosis and treatment of chronic wounds.
Objective: The aim of this study was to assess the wound healing benefits of a PVA Gelling Fiber by analyzing wound healing outcomes across a diverse sample of wound cases.
Methods: A retrospective review of published case studies was undertaken. Inclusions were any wound cases where a Polyvinyl (PVA) Gelling Fiber was used as the only primary dressing, regardless of the secondary dressing. A data collection form was designed and automated. Case contributions were 34 patients with 34 wounds, from 10 clinicians in 5 countries, over the course of 5 years. Patient, wound, and dressing performance data was collated and analyzed in aggregate form. Pre- and post-PVA gelling fiber patient and wound outcomes are compared and reported.
Results: For all patients, a silver (n=24) or non-silver (n=10) PVA gelling fiber was used as a primary dressing. Most wounds were changed weekly or bi-weekly, based on local protocols; supporting undisturbed wound healing for optimal wound healing with less frequent dressing changes. 64.7% of the wounds completely healed (n=22). The remaining wounds (n=12, 35.3%) were reduced in size and severity, with a mean area reduction of 95% and depth reduction of 91%. The mean duration of treatment was 7 weeks to healing (range of 2 weeks to 16 weeks), compared to a mean pre-PVA wound duration of 8.5 years . The overall condition of all wounds improved, as evidenced by a 142% increase in granulation and a 74.6% decrease in slough and eschar across all wound cases. Exudate levels for 88% of the wounds reduced to light (n=10) to none (n=20). All complications of sub-optimal care: dressing leakage and displacement, redness, biofilm, skin stripping, trauma, fragile skin, infection, and maceration resolved. Pain scores reduced to 1 or zero.
Conclusions: In this study, the use of a PVA gelling fiber as a primary dressing reduced pain, alleviated complications of care, reduced treatment time and healed acute and chronic wounds, even in patients with complex medical histories.

Poster #2
Skin Fails: Scoping the Evidence to Predict How & Why
Abstract: Background: Acute skin failure (ASF) is an elusive clinical phenomenon, commonly confused with other skin manifestations in the literature and in practice. The absence of clear guidance regarding ASF assessment, diagnosis, differentiation from other skin manifestations, treatment, and documentation can have negative implications for the patient, healthcare provider, and healthcare organizations.
Objective: The purpose of this scoping review was to map the use of Acute Skin Failure in the literature and to use identified patient characteristics to create point of care (POC) tools for assessment, differentiation, and documentation (ADD) of acute skin failure among adult and pediatric patients.
Methods: Scoping review using Arksey and O’Malley framework
Results: The search returned 2147 records. After limiters, exclusions for irrelevance, and duplicates were removed, seven studies across 196,878 adult (n=6) and pediatric (n=1) patients were included in the final analysis. Despite the assertion that there is no common or universally accepted definition of ASF, 6 of 7 studies used a common definition. This definition was used as the framework for categorization of statistically significant patient factors identified in the literature into two POC ASF-ADD tools. One focused on adult patients and one for pediatric patients.
Conclusion: Although this study adds clarity to the process acute skin failure identification, it also reveals substantial gaps in the current literature, the absence of tools to guide clear delineation of ASF from other skin manifestations. The ASF-ADD tool is a small step towards filling the gap for the nurse at the bedside, but more research is needed for ASF to be diagnosed, treated, and reimbursed like all of other organ failures.

Poster #3
Outcomes-Based Standardization: A New Approach to An Old Problem
Abstract: Background: The COVID-19 pandemic has significantly strained care delivery, reduced available resources, and further destabilized healthcare finances. As healthcare organizations emerge from a pandemic that created economic instability, reactive cost cutting with little regard for the people at the end of those decisions quickly emerged as the standard approach.1-6 In the post-COVID healthcare environment, where clinical and financial challenges are greater than ever, a new approach to reducing healthcare spending offers promise.2
Objective: Outcomes-Based Standardization is a new approach that begins with the end in mind. It incorporates lean concepts to alleviate redundant or ineffective products and practice, while prioritizing value added activities to catalyze the greatest reduction of harm, time, and money spent. The purpose of this project is to explain the Outcomes-Based Standardization Model, describe application of the model in practice to reduce hospital-acquired pressure injuries, and report successes across US hospitals.
Methods: Case-Based Proof of Concept
Results: Five cases are presented, demonstrating the real world application of Outcomes-Based Standardization in US hospitals. Each case is unique in its needs, goals, application of OBS, and outcomes achieved. Across the five cases, stock keeping units (SKUs) were reduced, waste was alleviated, and positive outcomes were achieved. These include hospital-acquired pressure injuries reductions ranging from 35.9% to 82.5% across the five cases. Stage 4 pressure injuries were reduced to zero and stage 3s reduced by 85% at one case site. 84 to 196 unnecessary length of stay days were avoided, and cost avoidance ranged from $438,000 to $1,371,321 for the case sites.
Conclusion: This new approach has been successfully employed across the country to help healthcare organizations achieve better clinical outcomes, alleviate waste, and reduce unnecessary healthcare spending.
![]()

Poster #4
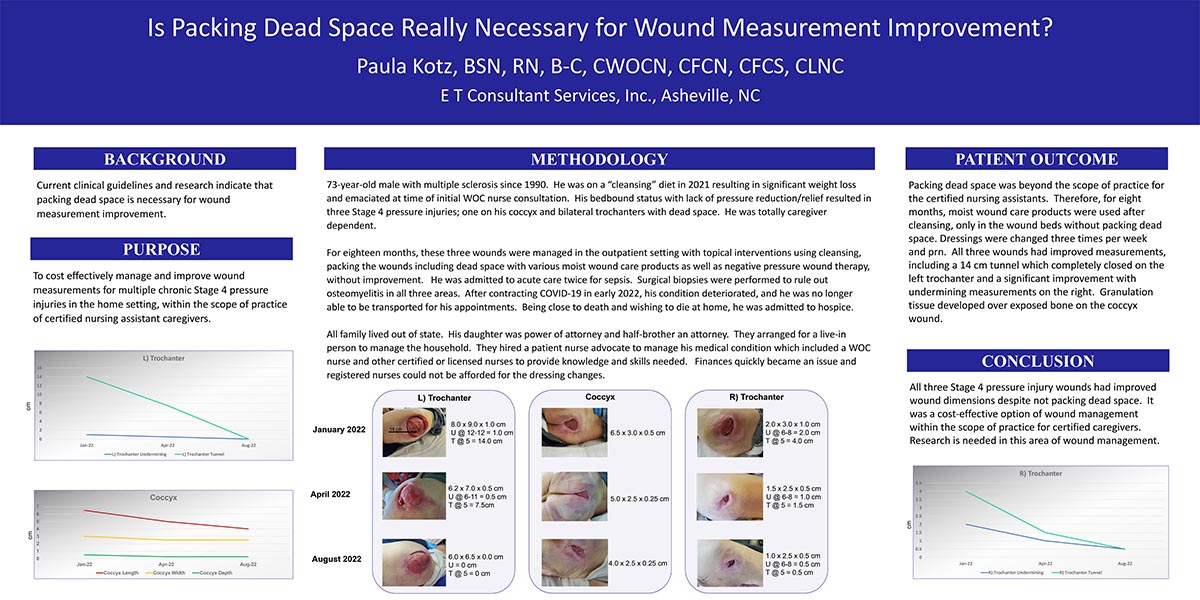
Is Packing Dead Space Really Necessary for Wound Measurement Improvement?
Abstract: Background: Current clinical guidelines and research indicate that packing dead space is necessary for wound measurement improvement.
Purpose: To cost effectively manage and improve wound measurements for multiple chronic Stage 4 pressure injuries in the home setting, within the scope of practice of certified nursing assistant caregivers.
Methodology: 73-year-old male with multiple sclerosis since 1990. He was on a “cleansing” diet in 2021 resulting in significant weight loss and emaciated at time of initial WOC nurse consultation. His bedbound status with lack of pressure reduction/relief resulted in three Stage 4 pressure injuries; one on his coccyx and bilateral trochanters with dead space. He was totally caregiver dependent.
For eighteen months, these three wounds were managed in the outpatient setting with topical interventions using cleansing, packing the wounds including dead space with various moist wound care products as well as negative pressure wound therapy, without improvement. He was admitted to acute care twice for sepsis. Surgical biopsies were performed to rule out osteomyelitis in all three areas. After contracting COVID-19 in early 2022, his condition deteriorated, and he was no longer able to be transported for his appointments. Being close to death and wishing to die at home, he was admitted to hospice.
All family lived out of state. His daughter was power of attorney and half-brother an attorney. They arranged for a live-in person to manage the household. They hired a patient nurse advocate to manage his medical condition which included a WOC nurse and other certified or licensed nurses to provide knowledge and skills needed. Finances quickly became an issue and registered nurses could not be afforded for the dressing changes.
Patient Outcome: Packing dead space was beyond the scope of practice for the certified nursing assistants. Therefore, for eight months, moist wound care products were used after cleansing, only in the wound beds without packing dead space. Dressings were changed three times per week and prn. All three wounds had improved measurements, including a 14 cm tunnel which completely closed on the left trochanter and a significant improvement with undermining measurements on the right. Granulation tissue developed over exposed bone on the coccyx wound.
Conclusion: All three Stage 4 pressure injury wounds had improved wound dimensions despite not packing dead space. It was a cost effective option of wound management within the scope of practice for certified caregivers. Research is needed in this area of wound management.
![]()
Poster #5
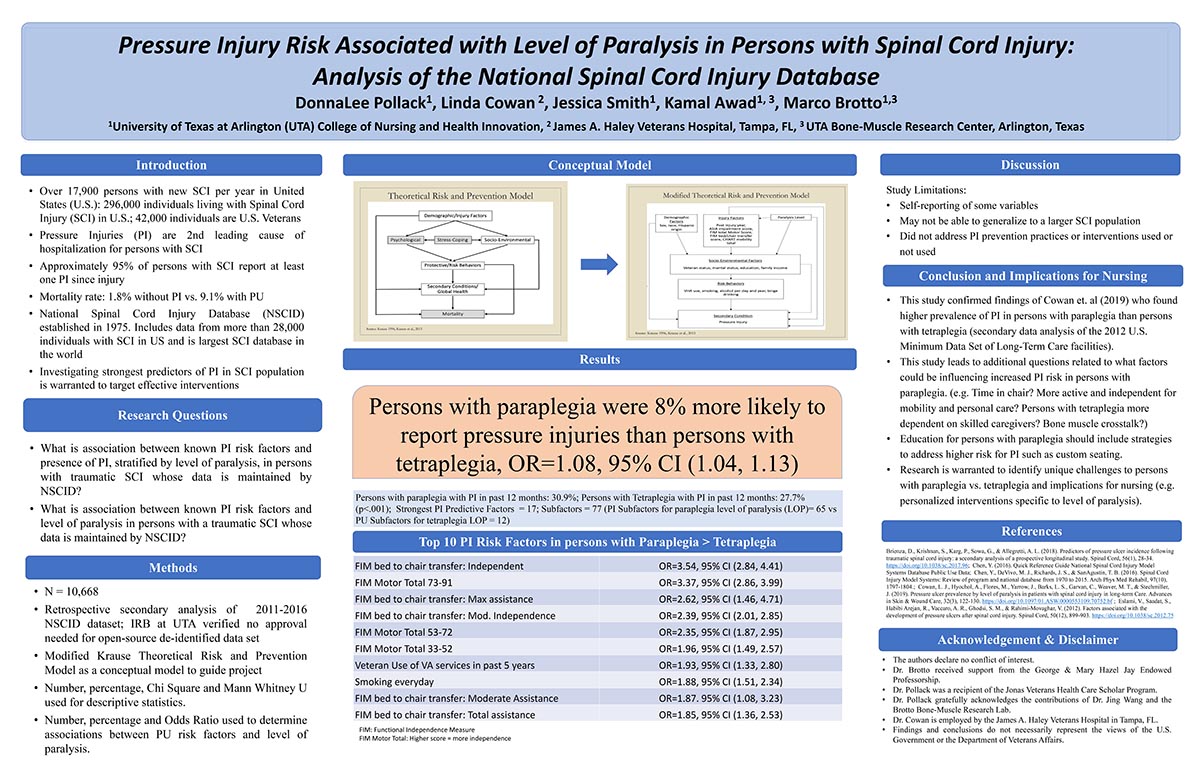
Pressure Injury Risk Associated with Level of Paralysis in Persons with Spinal Cord Injury: Analysis of the National Spinal Cord Injury Database
Abstract: BACKGROUND: Approximately 296,000 individuals are living with SCI in the United States (US). In persons with SCI, PI are the 2nd leading cause of hospitalization. Approximately 95% of persons with SCI report having at least one PI since SCI onset. Mortality rates are higher in persons with SCI and a PI (9.1%) versus SCI without a PI (1.8%). The National Spinal Cord Injury Database (NSCID) is largest SCI database in the world and was established in 1975. It includes 28,000 individuals with SCI in the US. Investigating strongest predictors of PI in SCI population(s) is warranted to target effective interventions.
PURPOSE: Determine associations between known PI risk factors and level of paralysis in persons with a traumatic SCI whose data is in the NSCID database.
METHODS: Retrospective secondary analysis of 2011-2016 NSCID de-identified dataset (N= 10,668). Descriptive statistics and logistic regression analysis used to describe associations between PI risk factors and level of paralysis.
RESULTS: Persons with paraplegia were 8% more likely to report pressure Injuries than persons with tetraplegia, OR=1.08, 95% CI (1.04, 1.13). Some of the top 10 PI risk factors in persons with paraplegia > tetraplegia were: 1. Functional Independence Measure (FIM) score for bed to chair transfer: Independent OR=3.54, 95% CI (2.84, 4.41); 2. FIM Motor Total 73-91 OR=3.37, 95% CI (2.86, 3.99); 9. Smoking everyday OR=1.88, 95% CI (1.51, 2.34
CONCLUSIONS: This study confirmed findings in other studies reporting higher prevalence of PI in persons with paraplegia versus tetraplegia. Research is warranted to identify factors influencing increased PI risk in persons with paraplegia (e.g. Time in chair? More active and independent for mobility and personal care and potentially risky behaviors such as smoking?) and implications for nursing (interventions specific to level of paralysis).
![]()
Poster #6
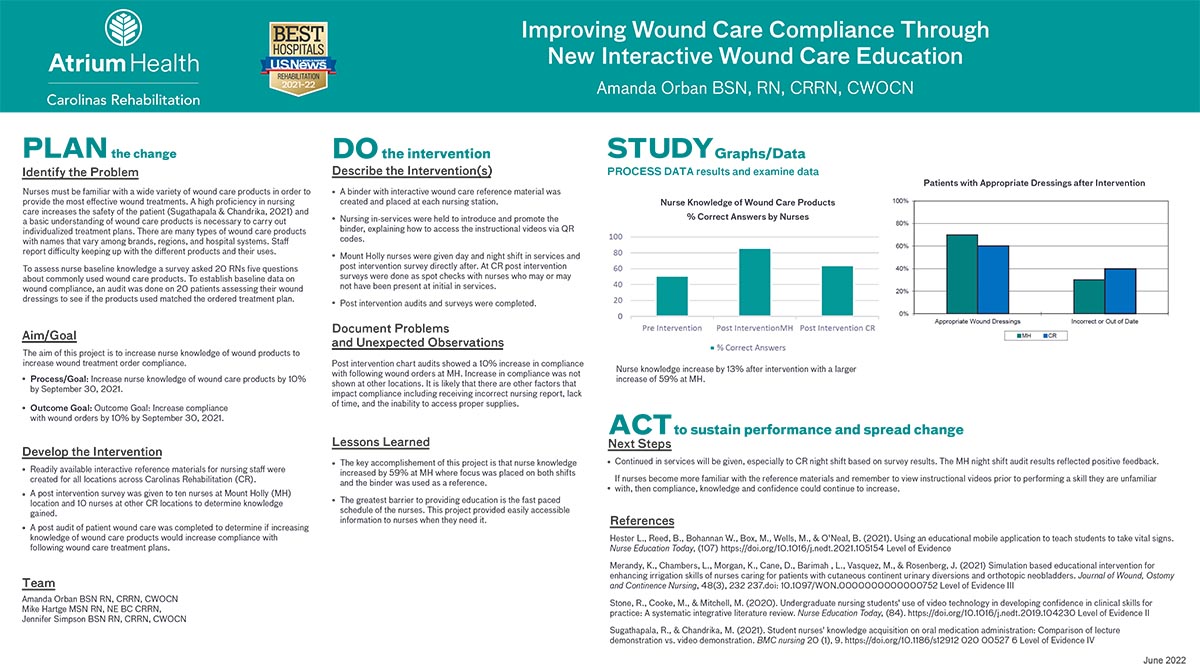
Improving Wound Care Compliance through New Interactive Wound Care Education
Abstract: Background: Nurses must be familiar with a wide variety of wound care products to provide effective wound treatments. A basic understanding of wound care products is necessary to appropriately carry out individualized treatment plans. There are many types of wound care products with names that vary between brands, regions, and hospital systems. Staff report difficulty keeping up with all the different products and their uses.
Objectives/Aim: The aim of this project was to increase RN knowledge of wound products to increase compliance with following wound treatment orders.
Methods: A survey was designed using a questionnaire completed by 20 nurses working in three inpatient rehabilitation facilities to establish baseline knowledge of wound care products and their uses. A readily available interactive reference binder of wound care information was created for nursing staff to access wound care information. A post intervention survey was given to 20 RNs at two of the inpatient rehabilitation locations to determine knowledge gained. A post audit of patients’ wound care was completed to determine if increasing knowledge of wound care products would increase compliance with following wound care treatment plans. Dressings were audited for appropriate product usage and time of change.
Results: Post-intervention chart audits showed a 10% increase in compliance with following wound orders at one of the facilities. Increase in compliance was not shown at other locations. Nursing knowledge of products increased by 13% at one facility and 59% at another facility where both day and night shift education was provided.
Conclusions. RNs can reduce the learning gap by becoming more familiar with wound care products and their proper uses. Nursing reported barriers including incorrect report, time constraints, and availability of supplies. The reference materials is a resource for RNs to access in their own time as the information is needed to perform tasks.
![]()
Poster #8
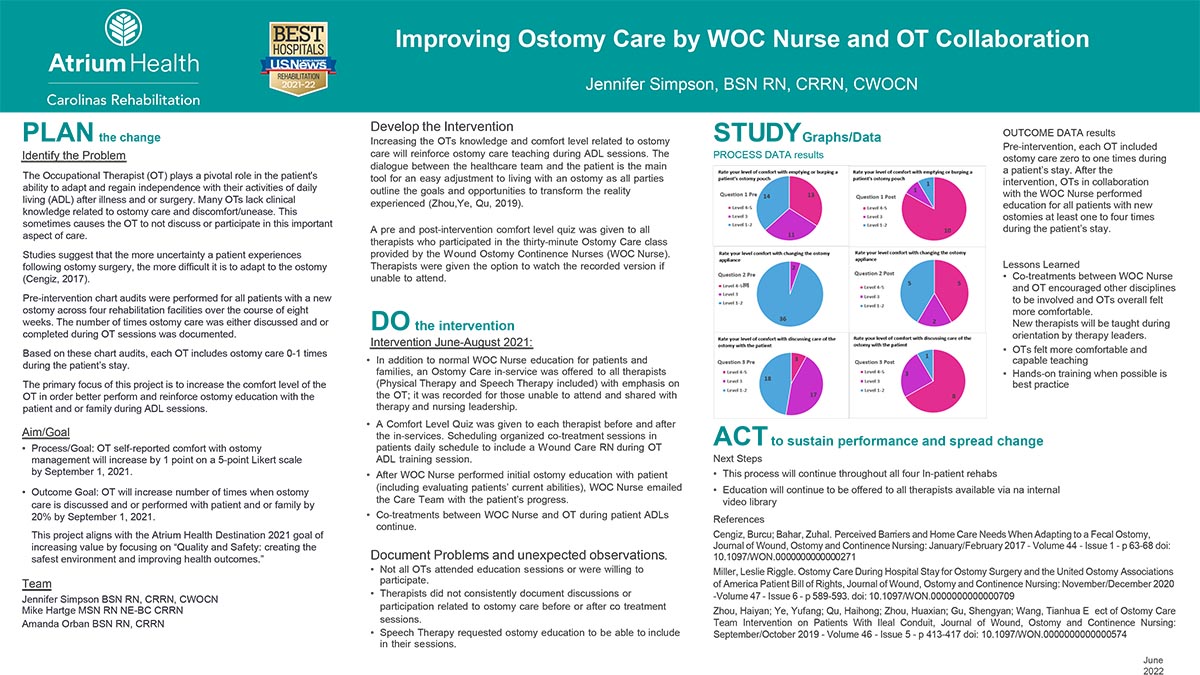
Improving Ostomy Care by WOC Nurse and OT Collaboration
Abstract: Background: The Occupational Therapist (OT) plays a pivotal role in the patient's ability to adapt and regain independence with their activities of daily living (ADL) after illness and or surgery. The primary focus of this project was to increase comfort level of the OT to better perform and reinforce ostomy education with the patient and or family during ADL sessions.
Purpose: The goal was for the OT to self-report comfort level with ostomy management to increase by 1 point on a 5-point Likert scale; and the OT would increase number of times ostomy care was discussed and or performed.
Method: The WOC Nurse provided four Ostomy Care in-services to therapists (Physical Therapist and Speech Therapist included) with emphasis on the OT role. Recordings were made available and shared with therapy and nursing leadership. In addition to in-servicing, WOC Nurse offered co-treatment sessions with OT during ADL training session.
In-servicing included education on how to burp, empty and change ostomy appliance. In addition to this ostomy products and accessories were reviewed to help familiarize staff.
A Comfort Level Quiz was given to each therapist before and after the in-services or recorded viewing. Approximately 38 participants completed the quiz pre-intervention and 12 post-intervention.
Results: Post-intervention, OTs reported a higher level of comfort as shown by the percentage who selected Likert 4-5 with burping (83% versus 34%), changing appliance (42% versus 0), and discussing with patients (67% versus 8%).
Pre-intervention, four patient chart audits showed each OT included ostomy care zero to one time during a patient’s stay. Post intervention, OTs included ostomy care for all 8 patients with ostomies one to four times during the patient’s stay.
Conclusions: Education and co-treatments with OT increased their comfort level and education reinforcement to patients and families.
![]()
Poster #9
Wound Hygiene: Utilizing Monofilament Pad for Multiple Uses in Long Term Care
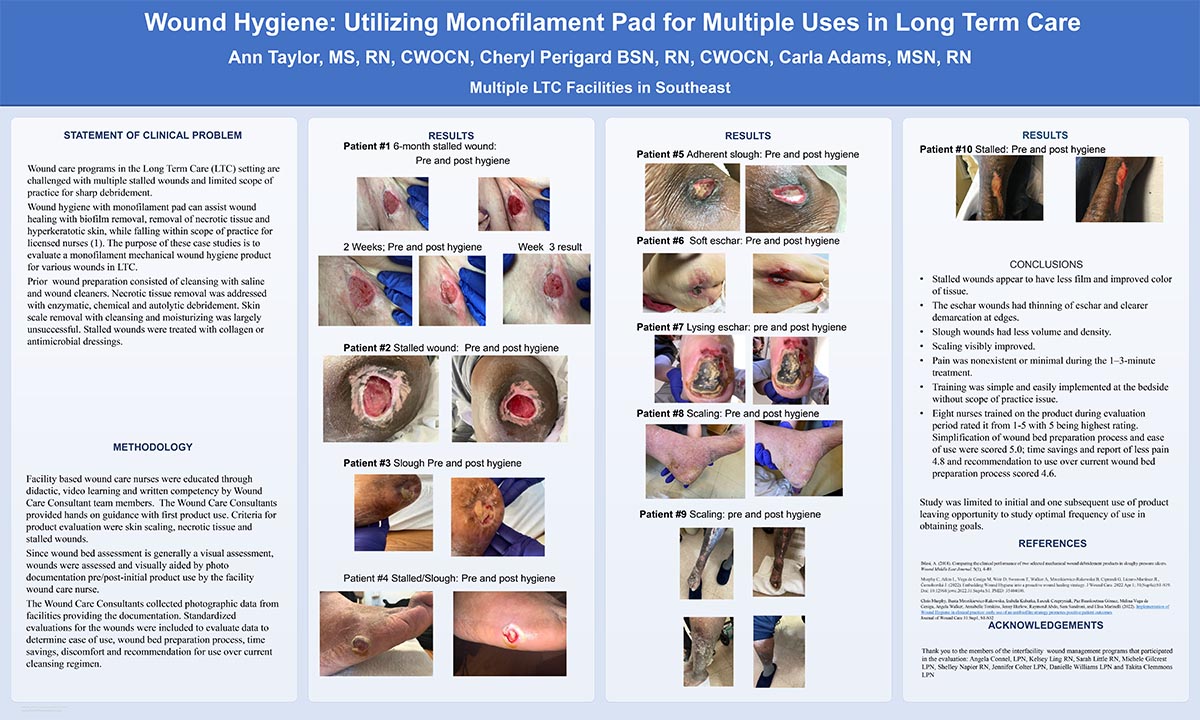
Abstract:Statement of Clinical Problem: Wound care programs in the Long Term Care (LTC) setting contend with stalled wounds and limited scope of practice for sharp debridement. Wound hygiene with monofilament pad impacts wound healing with biofilm removal, removal of necrotic tissue and hyperkeratotic skin, while falling within scope of practice for licensed nurses (1). The purpose of these case studies is to evaluate a monofilament mechanical wound hygiene product for various wounds in LTC.
Past Management: Wound cleansing was accomplished with saline and wound cleaners. Necrotic tissue removal was addressed with enzymatic, chemical, and autolytic debridement. Scale removal with cleansing and moisturizing was largely unsuccessful. Stalled wounds were treated with collagen or antimicrobial dressings.
Methodology: Facility based wound care nurses were educated through didactic, video learning and written competency by Wound Care Consultant team members. The Wound Care Consultants provided hands on guidance with first product use. Criteria for product use were skin scaling, necrotic tissue and stalled wounds. Since basic wound bed assessment is visual and the product is a wound hygiene product, the wounds were assessed by local facility nurse and aided by photo documentation pre/post-initial product use. The Wound Care Consultants collated pre and post treatment photographic assessment data in addition to standardized product evaluations to determine user satisfaction.
Outcomes: Ten patient case studies presenting with wound bed or skin scaling issues from multiple facilities were evaluated by photo documentation pre and post use of monofilament pad soaked with saline. Stalled wounds show the wound beds have less film and better color of tissue. The eschar wounds had thinning of eschar and clearer demarcation at edges. Slough wounds had less volume and density. Scaling markedly improved. Pain was nonexistent or minimal during the 3-minute treatment. Study was limited to initial and one subsequent use of product leaving opportunity to study optimal frequency of use in obtaining goals.
![]()
Poster #10
Treating Necrotizing Fasciitis with Gold Standard Advanced Therapies.
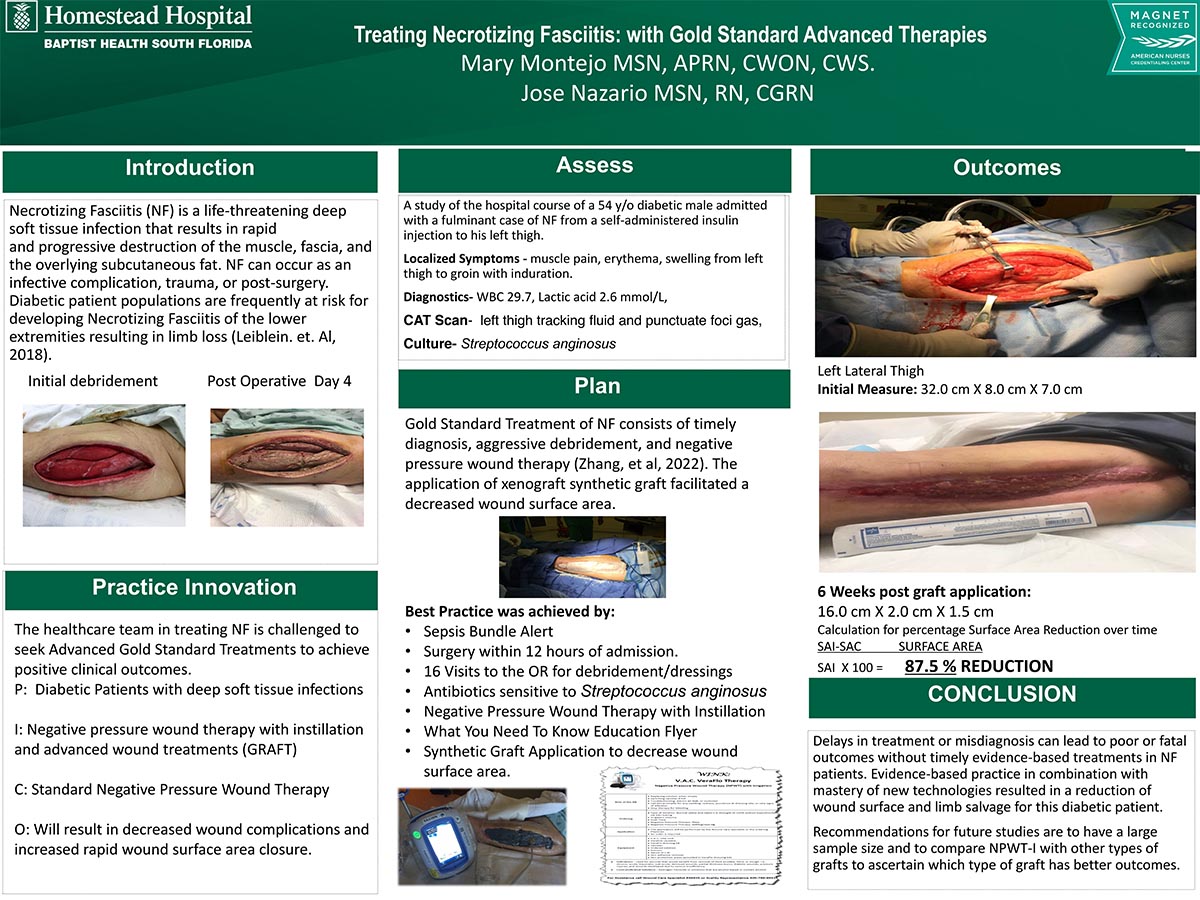
Abstract: Introduction: Necrotizing Fasciitis (NF) is a deep soft tissue infection that results in the progressive destruction of the muscle fascia and the overlying subcutaneous fat. NF can occur as an infective complication, trauma, or post-surgery. Its prognosis can be fatal, as high as 6% to 76% without timely evidence-based treatment (Zhang, Fan, Zhao, Shi, & Yu, 2021).
A study of the hospital course of an NF patient will be presented depicting two new innovative treatment modalities. The patient, a 54-year-old insulin-dependent diabetic male admitted c/o a left thigh abscess and cellulitis caused by a self-administered injection.
Practice Innovation: Standard wound care practice of NF patients post debridement includes the use of Negative Pressure Wound Therapy. An innovative therapy combination, Negative Pressure Wound Therapy with Instillation (NPWT-i), was selected because of the instillation/dwell properties coupled with granulation formation. NPWT-i has been found to assist in wound bed preparation and management of highly contaminated infected NF wounds (Zhang, Fan, Zhao, Shi, & Yu, 2021). A new xenograft synthetic graft application assisted wound closure of the large surgical full-thickness wound.
Outcomes: Evidence-based practice was achieved by adherence to the latest guidelines in NF treatment. The selection of two innovative treatment modalities; NPWT-i, and the synthetic graft placement facilitated wound closure and limb salvage. There was an 87.5% reduction in wound surface area.
Conclusion: Delays in treatment or misdiagnosis can lead to poor or fatal outcomes without timely evidence-based treatments in NF patients. Evidence-based practice in combination with mastery of new technologies resulted in a reduction of wound surface and limb salvage for this diabetic patient.
Future studies should consider a larger sample size and include a comparison of NPWT-i with different types of grafts to achieve better outcomes in the NF patient.
![]()
Poster #11
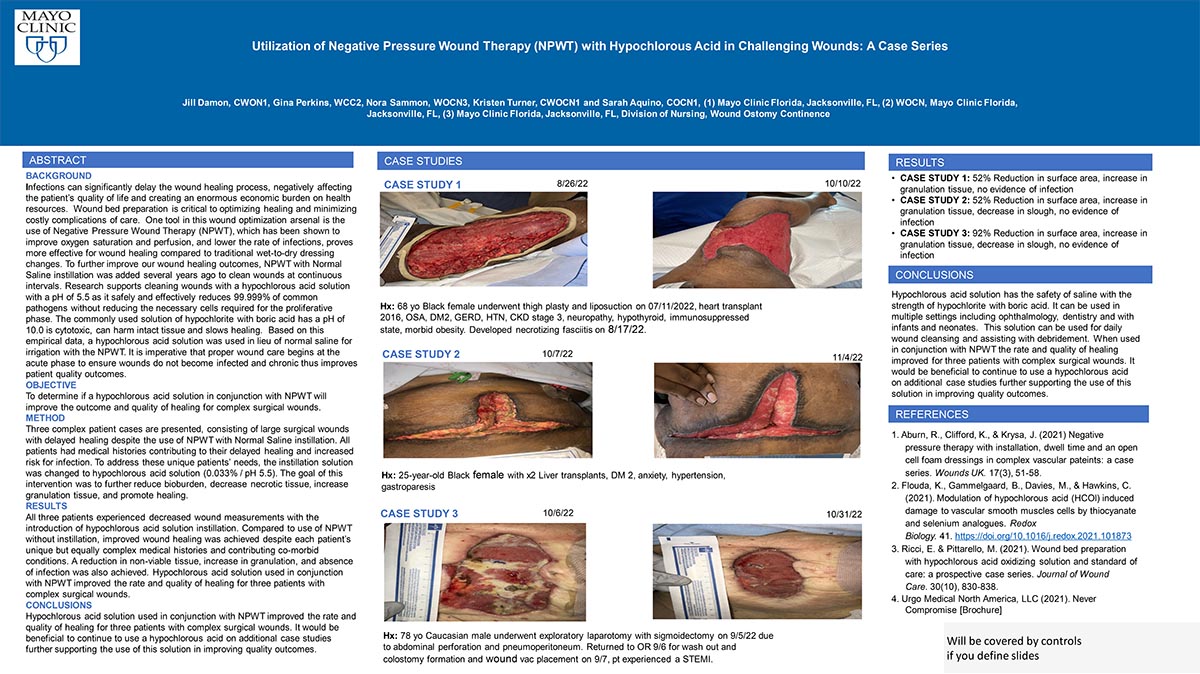
Utilization of Negative Pressure Wound Therapy (NPWT) with Hypochlorous Acid in Challenging Wounds
Abstract: Statement of Clinical Problem: Infected wounds have a significant impact on quality of life and carry a huge socioeconomic burden nationwide. Wound bed preparation is a critical component necessary for optimal healing including using wound cleansers to inhibit bacterial and biofilm formation. During the body’s natural inflammatory response, hypochlorous acid (HOCl) is generated by the heme enzyme myeloperoxidase (MPO) released by activated immune cells at the area of inflammation. Use of a hypochlorous acid solution which mimics the body’s natural response to inflammation has shown safe and effective as a wound cleanser.
Description of Past Management: It is imperative proper wound healing begins at the acute phase to ensure wounds do not become infected decreasing patient safety and quality outcomes. NPWT is standard practice for wound healing for full thickness wounds. A concern is for the patient to remain infection free. Previous wound management included NWPT without instillation, instillation with normal saline or sodium hypochlorite and boric acid in water.
Current Clinical Approach: Using a hypochlorous acid solution with a pH of 5.5 safely and effectively reduces 99.999% of common pathogens without reducing the necessary cells required for the proliferative phase
Three patients with large surgical wounds were treated with instillation negative pressure wound therapy and irrigation of a hypochlorous acid solution (0.033% / pH 5.5). These case studies provide supporting evidence of the effectiveness for the use of a hypochlorous acid cleanser as irrigate to reduce bioburden, decrease necrotic tissue and increase granulation tissue.
Patient Outcomes: All three patients saw a decrease in wound measurements during their hospital admission. All patients demonstrated improved healing under one month and one within 46 days. Two of the three patients also resulted in a decrease in non-viable tissue. All these patient’s wounds remained infection-free at time of discharge.
Conclusion: HOCI conjunctive use with NPWT improves healing, decrease in hospital stay and readmissions. Limitations are inability to utilize instillation outside of hospital and potential variations in measurements.
![]()
Poster #12
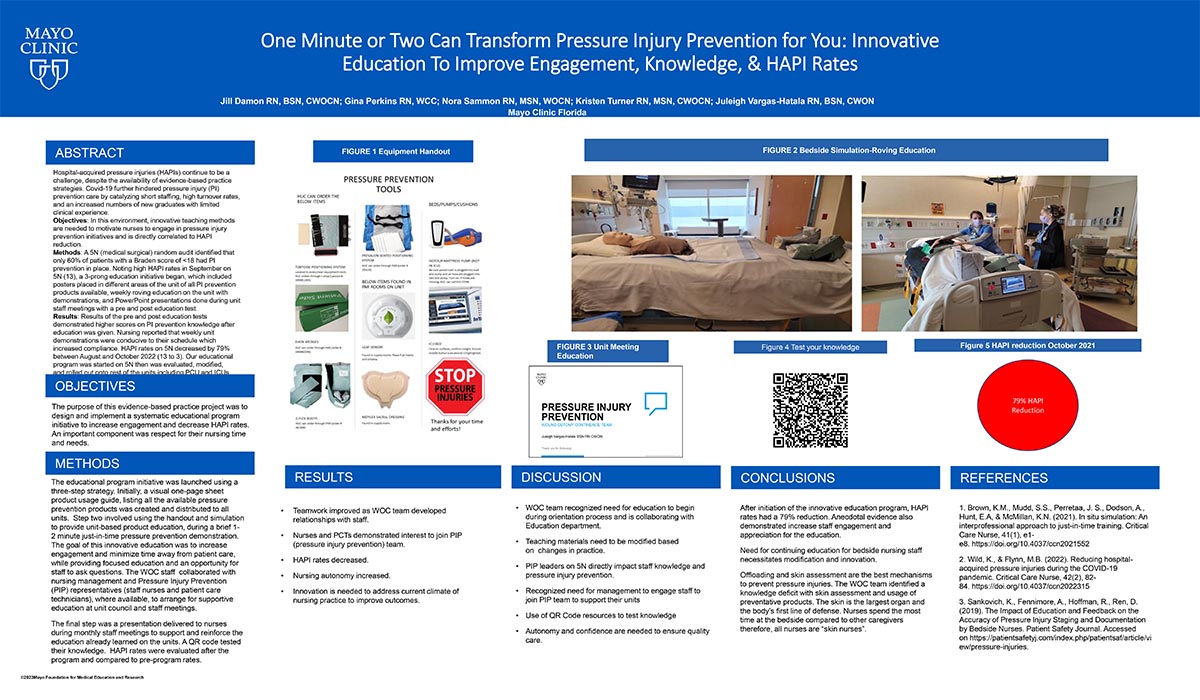
One Minute or Two Can Transform Pressure Injury Prevention for You: Innovative Education to Improve Engagement, Knowledge, & HAPI Rates
Abstract: Background: Hospital-acquired pressure injuries (HAPIs) continue to be a challenge, despite the availability of evidence-based practice strategies. Covid-19 further hindered pressure injury (PI) prevention care by catalyzing short staffing, high turnover rates, and an increased numbers of new graduates with limited clinical experience.
Objectives: In this environment, innovative teaching methods are needed to motivate nurses to engage in pressure injury prevention initiatives and is directly correlated to HAPI reduction.
Methods: A 5N (medical surgical) random audit identified that only 60% of patients with a Braden score of <18 had PI prevention in place. Noting high HAPI rates in September on 5N (13 for the month), a 3-prong education initiative began, which included posters placed in different areas of the unit of all PI prevention products available, weekly roving education on the unit with demonstrations, and PowerPoint presentations done during unit staff meetings with a pre and post education test.
Results: Results of the pre and post education tests demonstrated higher scores on PI prevention knowledge after education was given. Nursing reported that weekly unit demonstrations were conducive to their schedule which increased compliance. HAPI rates on 5N decreased by 79% between August and October 2022 (13 to 3). Our educational program was started on 5N then was evaluated, modified, and then rolled out onto rest of the units including PCU and ICUs.
![]()
Poster #13
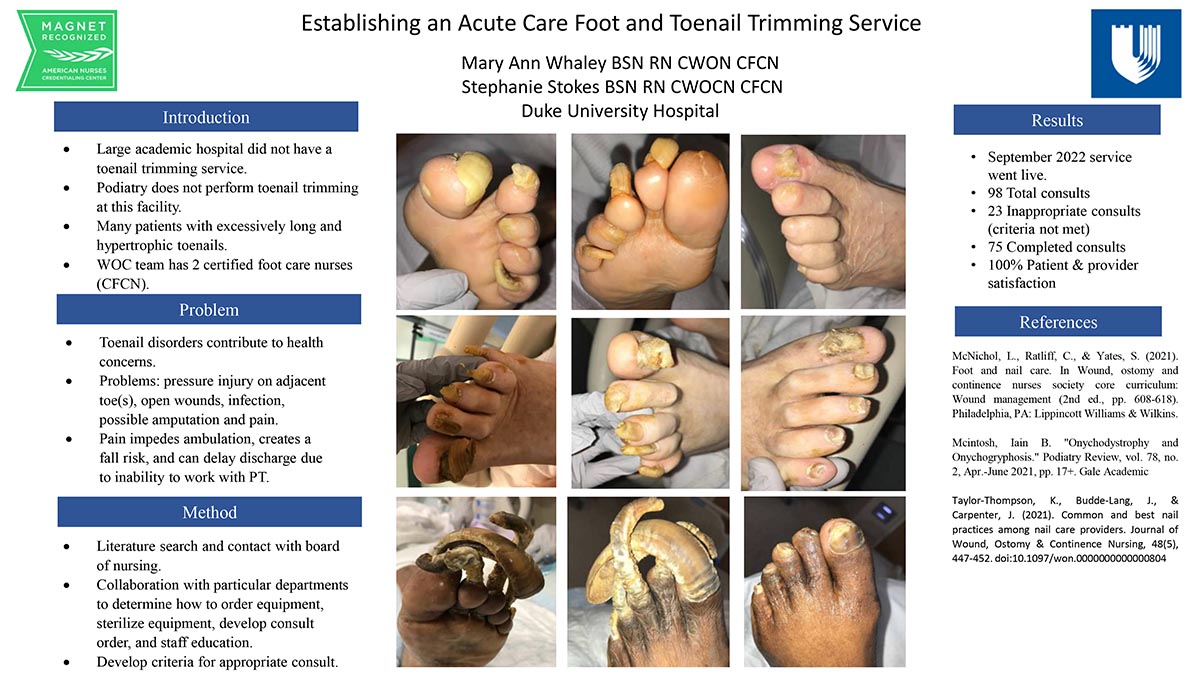
Establishing an Acute Care Foot Care and Toenail Trimming Service
Abstract: Introduction: In our large academic medical center, the WOC nurse team is frequently consulted for lower extremity ulcers including neuropathic foot ulcers. During the assessment, we note that many of the patients have excessively long and hypertrophic toenails. Our medical center did not have a toenail trimming service. We have 2 podiatrists and a nurse practitioner who do not provide routine toenail trimming. Our hospital has 2 certified foot care nurses (CFCN) who saw the need to fill this gap.
Purpose: Onychogryphosis can contribute to health concerns for patients. One of the problems is pressure on adjacent toes that can lead to open wounds, infection and possibly amputation. Long and misshapen nails can cause pain. The pain impedes ambulation, creates a falls risk and can delay discharge because a patient cannot work with physical therapy.
Method: Implementation of a foot care service began with a literature search and contacting the state board of nursing. Next steps included working with our procurement department to determine how to order needed equipment, working with our supply chain to discuss stocking of supplies, and emails to sterile processing to develop the process for sterilization of equipment. We also worked with the hospital Nursing Informatics Council for the consult build. The CFCNs collaborated with the clinical education department and the health system WOC Council to determine how we would educate the nursing and medical staff.
Results: In September 2022, the toenail trimming consult service went live. Since that time we have had 98 total consults. Of those, 23 were inappropriate (criteria not met), 75 were completed with 100% patient and provider satisfaction.
![]()
Poster #16
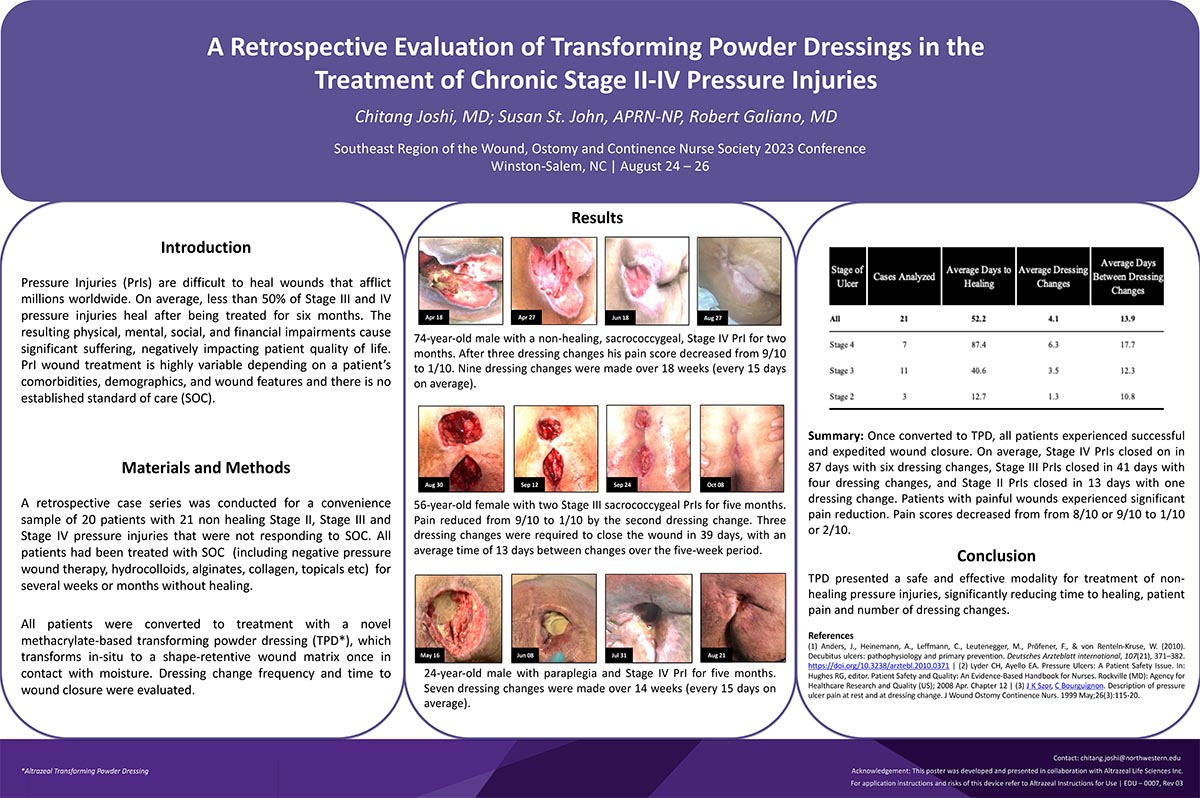
A Retrospective Evaluation of Transforming Powder Dressings in the Treatment of Chronic Stage 2-4 Pressure Injuries
Abstract: Introduction: Pressure Injuries (PrIs) are chronic, open wounds that continue to affect millions of adults worldwide. Along with physical impairment, patients are often affected mentally, socially, and financially. Treatment of PrIs is highly variable according to a patient’s comorbidities, demographics, and wound characteristics, and, because of this, there exists no standard dressing for PrIs. Transforming powder dressing (TPD) is a promising new form of wound treatment; however, little evidence exists for TPD in chronic PrIs. This case series sought to examine the effect of TPD in chronic PrIs which have previously undergone unsuccessful standard of care wound therapy.
Materials and Methods: This retrospective case series used data from a convenience sample of 20 patients with 21 nonhealing Stage II, III, and IV wounds that failed to heal with standard of care therapies (including negative pressure wound therapy, hydrocolloids, alginates, collagen, topicals, etc). All patients were converted to treatment with TPD, which transforms in-situ to an extended wear (up to 30 days) shape retentive wound matrix once in contact with moisture. Factors examined were number of dressing changes, time between dressing changes, time to wound closure, and pain level. While data was assessed from all 21 patients, we focused on three particular cases that most clearly illustrated TPD’s effect on wound healing.
Results: Each patient experienced successful wound closure, with stage 4 taking an average of 98 days with 6 primary dressing changes, stage 3 having an average of 40 days to closure with 3 dressing changes, and stage 2 with 13 days to closure with 1 dressing change. Specifically, our three cases each showed reduction in pain from an 8 or 9 out of 10 to a 1 or 2 within the first dressing change.
Discussion: Pressure injuries that had previously failed to heal from standard of care interventions healed once patients were converted to TPD. TPD presented a safe and effective modality for treatment of nonhealing pressure injuries, significantly reducing time to healing, patient pain, and number of dressing changes. We suggest future prospective studies in order to more effectively measure the wound healing capability of TPD in pressure injuries.
Trademarked Items (in Footnote): Altrazeal® Transforming Powder Dressing (Altrazeal Life Science Inc.)
![]()
Poster #17
Patient-centered Ostomy Toolkit: An Approach to Standardize Care and Education of Patients with a New Ostomy
Abstract: Title: Patient-centered Ostomy Toolkit: An Approach to Standardize Care and Education of Patients with a New Ostomy
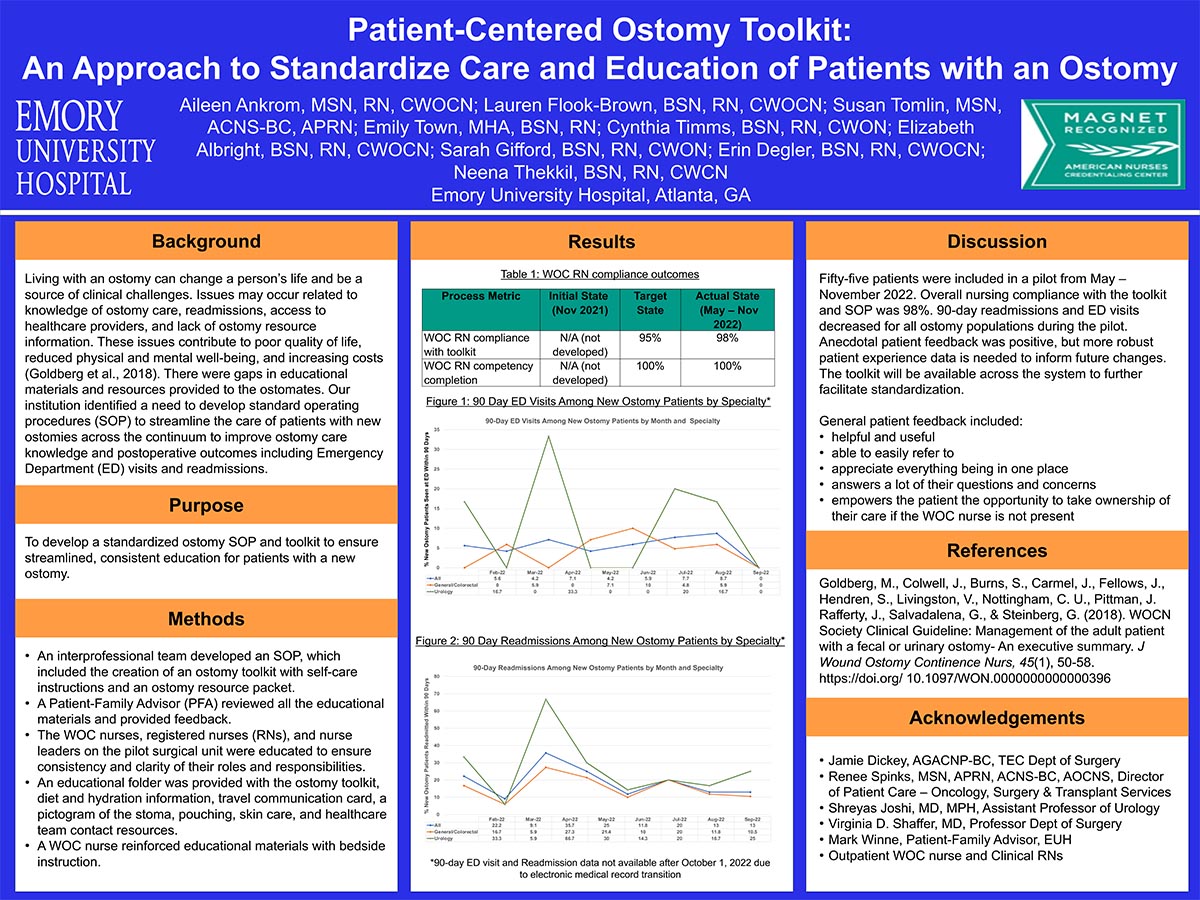
Abstract: Background: Living with an ostomy can change a person’s life and be a source of clinical challenges. Issues may occur related to knowledge of ostomy care, readmissions, access to healthcare providers, and lack of ostomy resource information. These issues contribute to poor quality of life, reduced physical and mental well-being, and increasing costs (Goldberg et al., 2018). There were gaps in educational materials and resources provided to the ostomates. Our institution identified a need to develop standard operating procedures (SOP) to streamline the care of patients with new ostomies across the continuum to improve ostomy care knowledge and postoperative outcomes including Emergency Department (ED) visits and readmissions.
Purpose: To develop a standardized ostomy SOP and toolkit to ensure streamlined, consistent education for patients with a new ostomy.
Methods: Interprofessional team developed an SOP, which included the creation of an ostomy toolkit with self-care instructions and an ostomy resource packet. A Patient-Family Advisor (PFA) reviewed all the educational materials and provided feedback. The WOC nurses, registered nurses (RNs), and nurse leaders on the pilot surgical unit were educated to ensure consistency and clarity of their roles and responsibilities. An educational folder was provided with the ostomy toolkit, diet and hydration information, travel communication card, a pictogram of the stoma, pouching, skin care, and healthcare team contact resources. A WOC nurse reinforced educational materials with bedside instruction.
Results and Discussion: Fifty-five patients were included in a pilot from May – November 2022. Overall nursing compliance with the toolkit and SOP was 98%. 90-day readmissions and ED visits decreased for all ostomy populations during the pilot. Anecdotal patient feedback was positive, but more robust patient experience data is needed to inform future changes. The toolkit will be available across the system to further facilitate standardization.
![]()